 ONE OCTOBER DAY in the fall of my junior year of college, I found myself sitting in a chair across from a small blond woman with a look of deep concern on her face as she stared into mine. She had something to tell me, she said, and it was clear she knew that the something would upset me. Her eyes were wide, her hands on the arms of a chair that would have been more appropriate in a public library lounge. Her windowless office was warmly lit with a few small lamps, none of the bright fluorescence and antiseptic shine of a doctor’s office. Still, it was a doctor’s office, or at least it was an office in which something resembling medical care was taking place, and I had the feeling she was about to tell me that mine could no longer take place here.
ONE OCTOBER DAY in the fall of my junior year of college, I found myself sitting in a chair across from a small blond woman with a look of deep concern on her face as she stared into mine. She had something to tell me, she said, and it was clear she knew that the something would upset me. Her eyes were wide, her hands on the arms of a chair that would have been more appropriate in a public library lounge. Her windowless office was warmly lit with a few small lamps, none of the bright fluorescence and antiseptic shine of a doctor’s office. Still, it was a doctor’s office, or at least it was an office in which something resembling medical care was taking place, and I had the feeling she was about to tell me that mine could no longer take place here.
I was right, but for the wrong reasons. At 20, a good student from a good suburban family, I felt I had no right to sit there and lament to a professional who was here purely to solve the hardest of personal problems. I knew she was about to tell me I had to go, that there were precious few time slots available and I was taking one from someone who actually needed it.
Instead she looked at me with that genuine concern, and told me, gently, that she suspected my troubles were not something she could address in the 12 free sessions university students were allotted at the counseling center, that I needed someone who could help me long term if I were to ever stop crying in front of near strangers, if I were to ever get better.
That moment in her office turned into months, then years, of starting and stopping treatment, of bouncing between doctors, searching for the single thing at the bottom of it all: the one memory, the one trauma, the one blemish on my makeup that could explain everything, that could be wiped away to make me a happy person. That is how I had come to understand mental illness, as a simple disease that could be treated if only one could figure out what the disease was.
HAPPINESS, YOU MAY HAVE LEARNED earlier than I, is not like that. Nor is mental illness. At 29 years old, I have received many diagnoses since that day in the windowless office, but as various symptoms have risen and subsided, so too has the diagnosis with which I most identify. If you try to assign an illness to each manifestation of your problem, you can end up with a jumble of names that contains both too much and too little information, like a grocery list that notes all the dishes one hopes to make but none of the ingredients with which to make them.
In fact, modern mental health diagnosis has had at least as much to do with getting care paid for as with providing good care in the first place. The Diagnostic and Statistical Manual, Mental Disorders–a text that has become what is often referred to as the bible of psychiatry–arose in the aftermath of World War II, creating the outlines of professional psychiatric and psychologic practice that still exist today. “The manual was also the first to define what a mental disorder is,” writes University of Maryland psychiatrist Bernard A. Fischer in his history of mental illness diagnostic practices, “which was tremendously important in legitimizing the field as a medical specialty.”
Five decades later, we still have not found a diagnostic and treatment system that accurately reflects the lived experience of mental illness. In 2014, psychiatrist Martha Stout noted in her review of Gary Greenberg’s history of the DSM that its overseeing organization, the American Psychiatric Association, “stands accused of attempting to include under the purview of psychiatry many of the natural and normal forms of suffering, such that doctors may diagnose more illnesses and prescribe more medications….we use a diagnostic system we don’t respect to bill insurance companies for our patients.”
WE HAVE, I THINK, improved in one area, and that is in treating those afflicted with respect, decency, and the seriousness of scientific inquiry. Fewer, I hope, are the individuals who have a particularly bad bout of depression or a hallucination or two–a mental state the great Oliver Sacks called “an essential part of the human condition”–and find themselves condemned to a life in an understaffed psychiatric ward.
But much of that progress has been inextricably linked to equating emotional suffering with physical suffering, and that is entirely missing the point. Depression and its ilk are not worthy of attention, care, and compassion because they are medical problems; they are worthy because they cause human suffering, because emotional pain is just as real as physical.
The point is not that mental illness is not a medical issue. The point is that it is not only a medical issue, and more importantly, that treating it as such has serious consequences for the lives of patients, their families, and everyone else. This reductionist approach creates a misleading impression that mental illness is entirely like cancer, or a broken leg, or strep throat, in that you either have it or you don’t and there is some standard or test, not open to interpretation, by which we can determine who is who. That impression is a barrier to care for people who may feel they do not meet an often arbitrary standard of illness.
When I sat in that chair as a terrified teenager, it meant everything to have someone with a degree legitimize my problem, as though my pain weren’t real until a professional deemed it so. As I slogged through treatment throughout my early 20s, receiving a more severe diagnosis felt like, if not quite a badge of honor, at least a recognition of time served. (“Everyone’s depressed,” I happily told one therapist after receiving a Bipolar II diagnosis, feeling I’d at last been marked a true sufferer.) Terrifying as the thought is now, I used to wish for hallucinations, as they seemed a clear and unambiguous signal that I was capital-s Sick and would not be seen as somehow weak or unable to make it in this world if I took time off to take care of myself. Self-harm has many motivations, but one of them is to make physical that which feels too intangible for the rest of the world to take seriously.
IN THE 1990s, physician Nortin Hadler made the astute observation that a person forced with proving the reality of her illness can’t possibly hope to improve. A rheumatologist and immunologist, he was referring to chronic pain and the mystery of fibromyalgia, but his point applies equally well to mental illness.
Our public conversations about mental illness reveal a desire to sort folks into ill or not. Instead, we should work to communicate that mental health operates more like a spectrum, that we all will find ourselves at different points of that spectrum during different times in our lives, and that anyone is deserving of the insights of a professional. And we can take a cue from practices that have proven effective in psychotherapy: talking about what’s bothering us, and listening when someone else does so.
A few years ago, I spent some time in a therapy group with a woman who experienced regular sexual abuse from an adult family member during her childhood and adolescence. I met her in her 40s, after she had spent decades in various forms of treatment. When the holidays neared she spoke about being troubled by interactions with her mother, who refused to accept that the abuse had happened, a denial that made it difficult for my friend to spend time with her family. She struggled with whether to speak up: She missed her mother, but also felt that, with her mother in her 70s, perhaps it was too late for a confrontation. Perhaps she should simply wait it out.
From my seat in the circle, the solution seemed obvious. This person had been robbed of her childhood and adolescence and had spent her entire young adulthood dealing with the fallout. She had been forced into so many years of pain and deserved, perhaps more than anyone I’ve ever met, to put herself first, to make others’ lives more difficult or uncomfortable if it meant improving hers. It was so easy to see in her something that I’d never recognized in myself, that tendency to remove one’s own needs from the equation, to see oneself as at best a passive player in a game that exists for everyone else. In truly listening to another, I healed a part of myself.
________
Laura Dattaro is a freelance science writer who particularly likes space, physics, and philosophy.
________
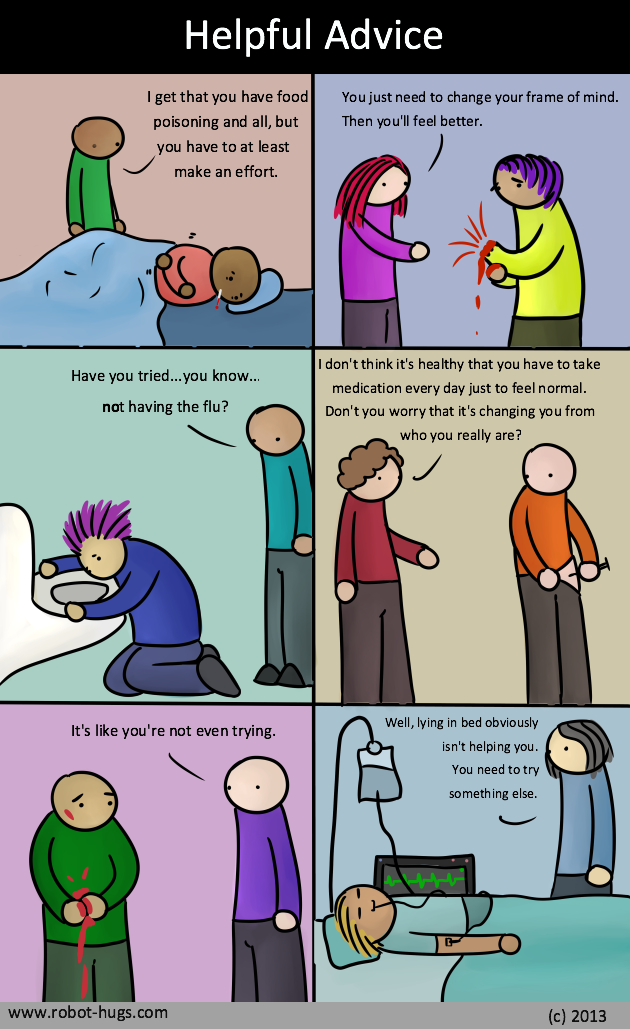
Helpful Advice cartoon by Robot Hugs whom we thank for making their art Creative Commons
4 thoughts on “Guest Post: The Non-Simplicity of Mental Illness”
Comments are closed.